


Region scanned:
Maxilla and mandible, the nasal cavities and paranasal sinuses, including parts of the skull base, upper cervical spine and pharyngeal airway
Reason for referral:
Implant placement in UL4, UL5, UL6 and LL6 sites. Assessment of bone and sinuses including patency of ostio-meatal complex
Scanner used:
KaVo OP 3D V17
Radiation dose:
Approximately 0.17 mSv
View the full scan using the links below:
i-CAT Vision  (caseoftheweek24)
(caseoftheweek24)
*NEW!!! Xelis Dental  (full implant library)
(full implant library)




Findings:
Maxillary antra, nasal cavities and other paranasal sinuses:
There is coverage of all the nasal cavities and paranasal sinuses apart from the most superior parts of the frontal sinuses. There is deviation of the nasal septum to the right side, with a bony spur projecting into the right middle meatus. Asymmetries of the turbinate bones are associated with this, with relatively larger turbinates on the left side and with a paradoxical curvature of the left middle turbinate. No mucosal disease in the nasal cavities. The maxillary antra are aerated normally apart from very limited mucosal thickening at the medial part of the antral roof on the right side, close to the natural ostium. The ostia are patent bilaterally (image 1). Other paranasal sinuses are normally aerated. The deviation of the nasal bone anatomy has an effect on the width of the frontal recess (the drainage channel of the right frontal sinus leading into the ostio-meatal complex), but it is patent. Overall, the ostio-meatal complexes are patent bilaterally and the nasal cavity and paranasal sinus health is clear.
Jaws and teeth:
Periodontal bone levels are mainly normal or show mild bone loss, but there is greater bone loss associated with UR8 and UR7 and incidental finding of caries. UL4, UL5, UL6 sites have a mature alveolar ridge. No retained roots or bony pathosis. Selected images 3 are bucco-palatal cross-sections across the site. Bone height to the antral floor steadily falls moving distally across the site. There is a short transverse septum at the maxillary antral floor above the palatal side of UL5 site, which should not be relevant to any sinus lift procedure being planned. The alveolar bone quality appears satisfactory, with fairly dense trabeculation and well-defined cortices. The LL6 site has a mature alveolar ridge with no retained roots or bony pathothis. LL7 is mesially inclined, so that its crown overhangs the site. Selected images 4 are bucco-lingual cross-sections across the site. The alveolar ridge has a broad crest. There is a mild lingual undercut, with a lingual concavity present mesially in the site and in the premolar region. The lingual concavity of the submandibular fossa appears towards the distal end of the site. The ID canal is easily identified, lying quite low in the bone. The mental canal is in the plane of LL5. Bone quality is satisfactory, with well-defined thick cortices and fairly evenly trabeculated medullary bone.
Normal bony anatomy of facial bones, including the TMJs. Normal upper cervical spine.
Image 1
Coronal cross-section through the maxillary antra and their ostia
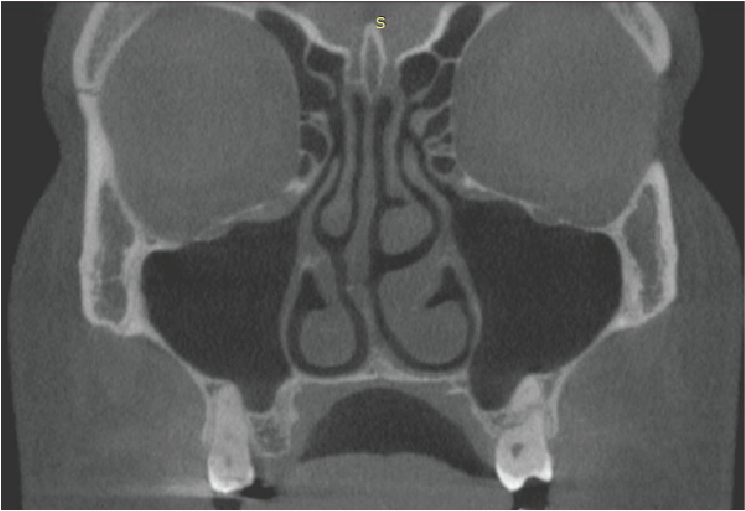
Image 2
Panoramic reconstruction
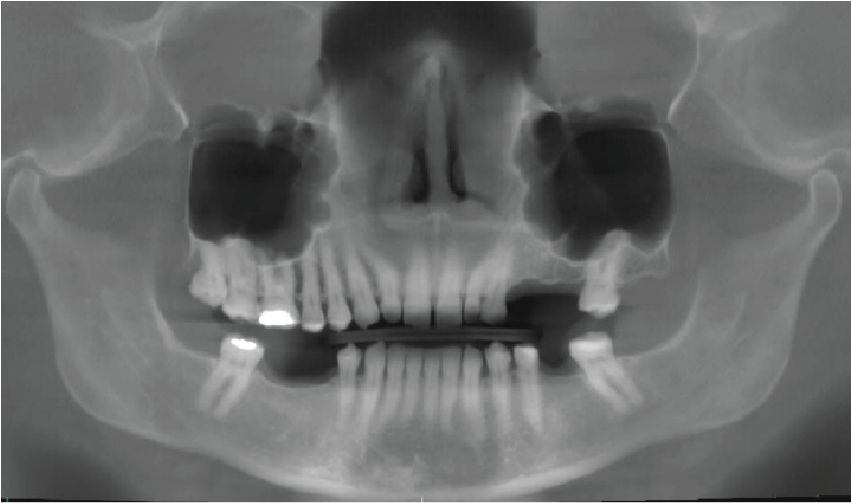
Image 3
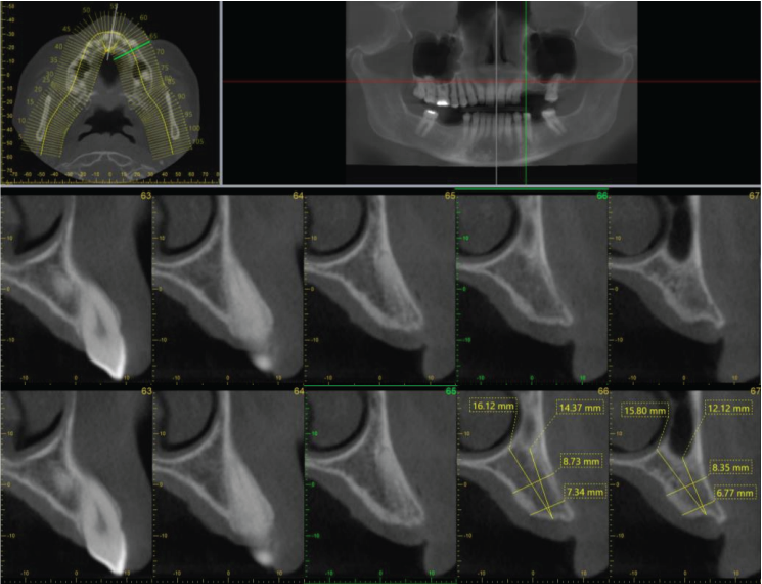
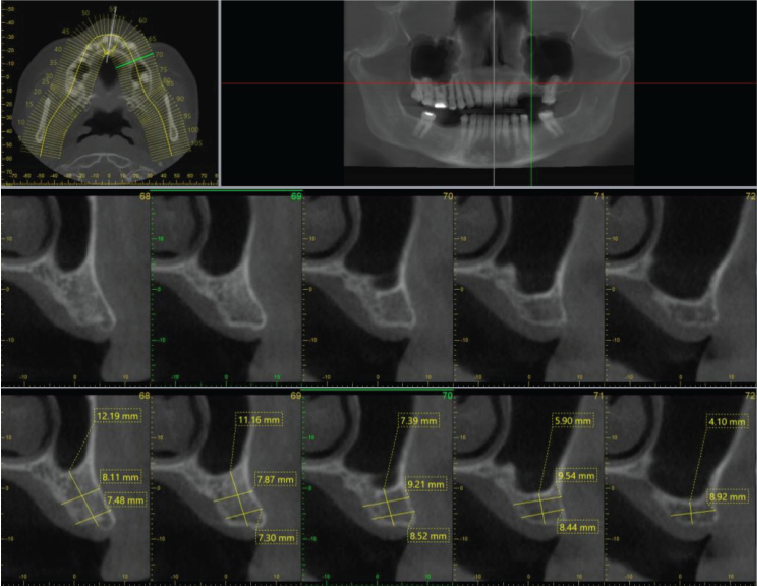
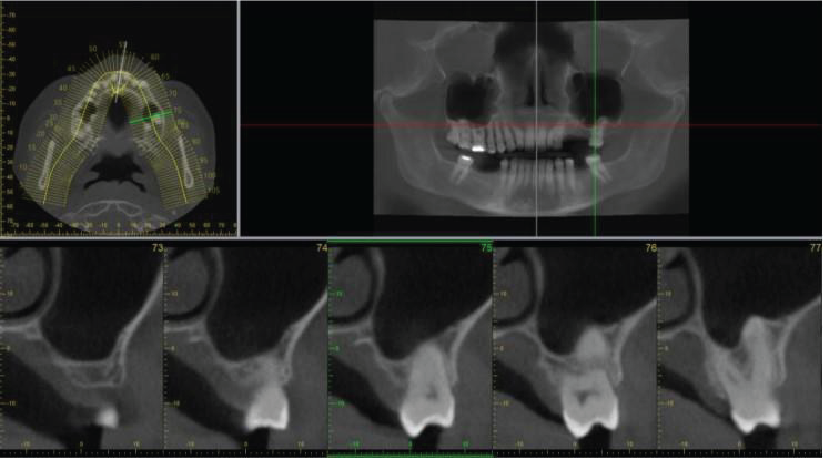
Image 4
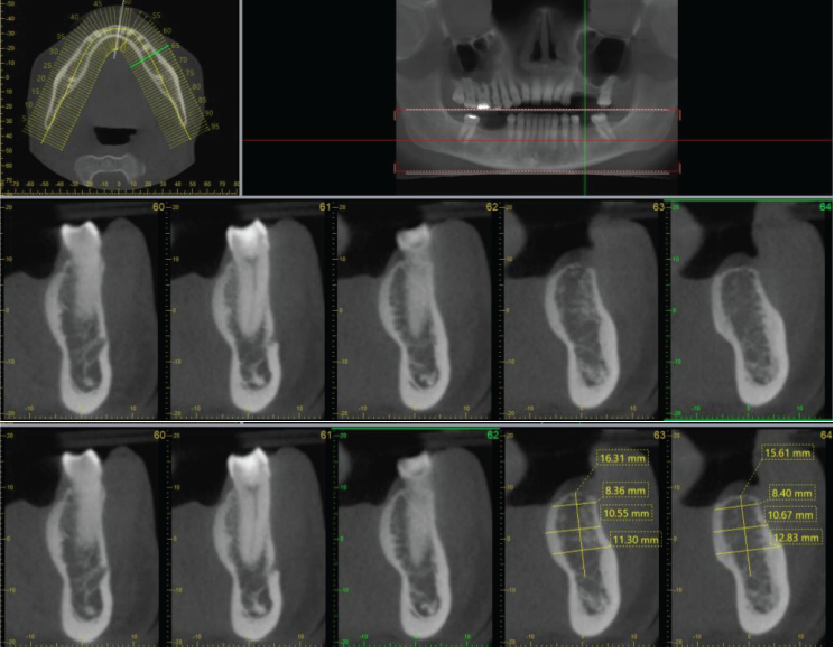
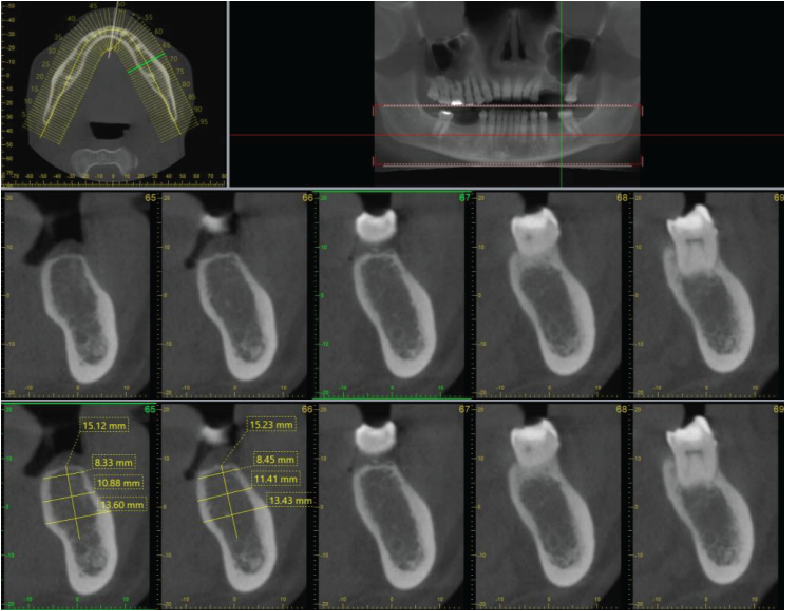
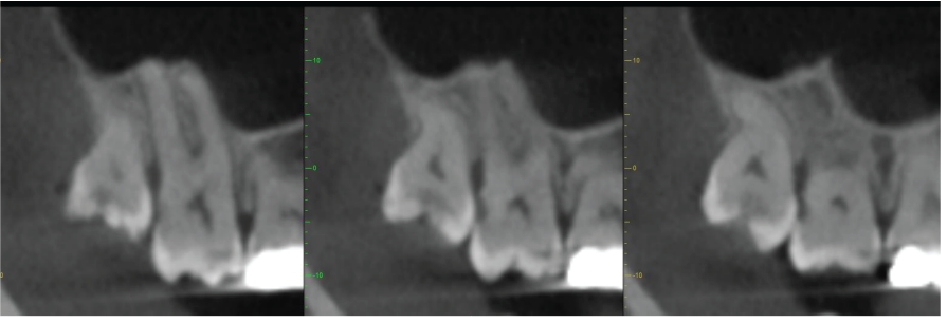
Image 5
Mesio-distal cross-sectional images UR8 and UR7, showing the caries and the distal periodontal bone loss on UR7
|

View our other cases 👉 Cases of the week │ Contact Us │ Locations │ Online Bookings

