

Recently I received a small volume quadrant scan of the right maxilla of a 50-year-old man. The clinical information provided was “Please assess scan prior to implant placement in UR4 site.”
Initial examination of the scan volume with a coronal slice through the R cheek, maxillary sinus and nasal septum revealed 1) Absent R lateral wall of nose, 2) Absent R lateral wall of maxillary sinus.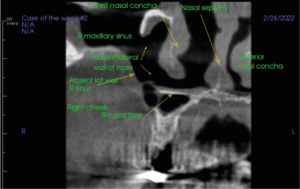
Figure 1. Coronal section Right cheek and maxillary sinus
An axial slice (left image in Figure 2) shows an incomplete well defined unilocular radiolucency 3 x 2 mm in the buccal side of the alveolar ridge UR 5 edentulous region (circle in image). Just posterior in UR6,7 region there is a well-defined unilocular radiolucency 9 x 4 x 7 mm (single arrow) with loss of boney outline (two arrows). In the sagittal slice, right image of Figure 2, UR5 radiolucency shows a loss of the maxillary sinus boney floor.
From the appearance of the radiographs, I could deduce the following:
- The missing bone in the nose had clear cut margins, typical of surgery
- The missing bone in the lateral wall of the Right maxillary sinus could be from surgical access to the sinus
- Disease was present in the buccal cortical plate region of the Right posterior alveolar bone ridge
- The cyst-like radiolucency was not encapsulated completely by bone as the anterior
portion of the “cyst” had thinning/ loss of the bone cortex. - Generally, the bone of the sinus and alveolar ridge did not have poorly defined “moth-eaten” bone typical of malignancy
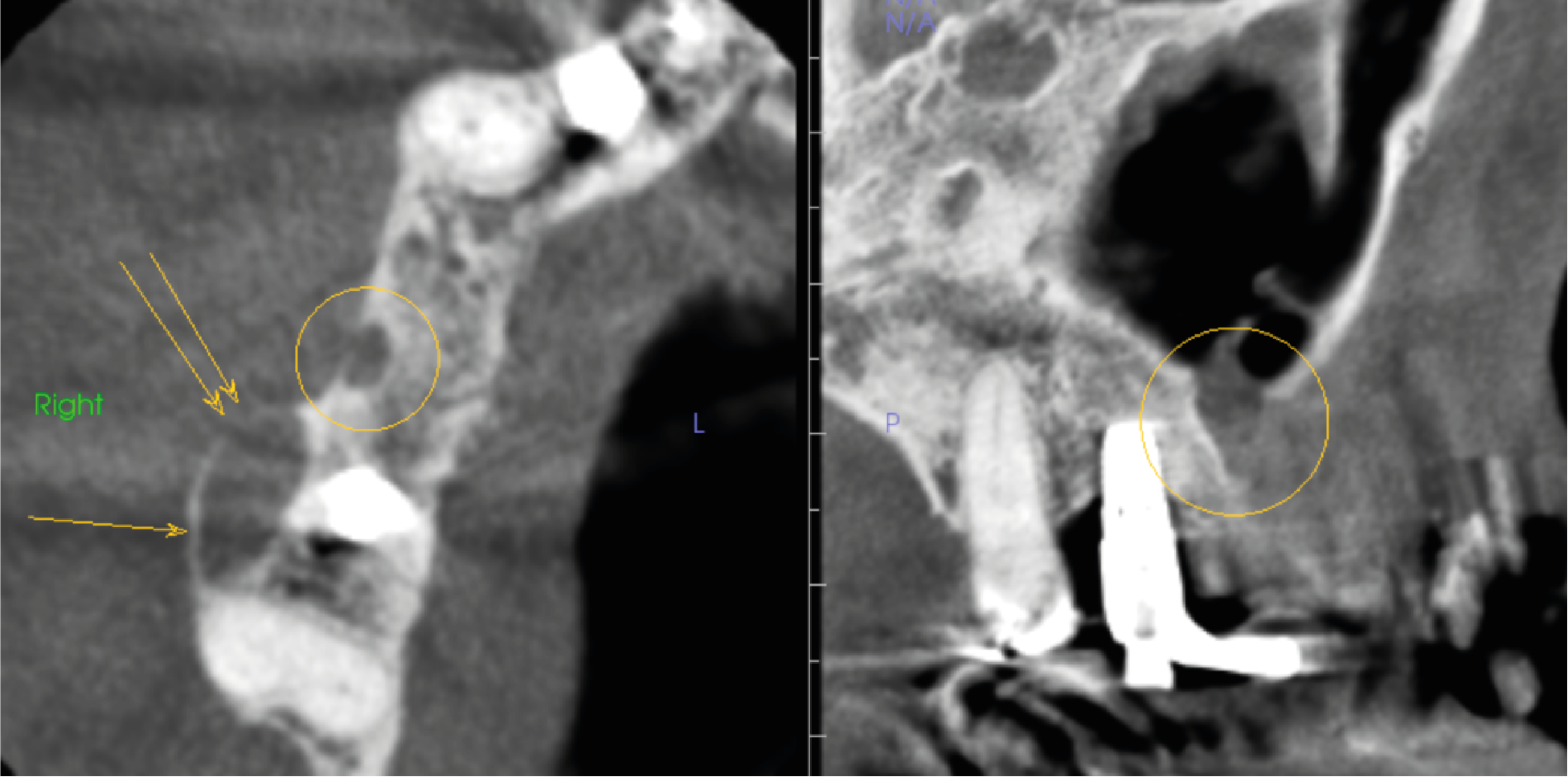
Figure 2. Right image is axial slice through UR alveolar bone ridge with circle in UR5 region and arrows UR6 region. Left image is sagittal slice UR7 to UL3 region
It was clear to me that the patient had previously received surgical treatment of the right maxilla. The question was, why? Could the cystic lesion on the alveolar ridge be new disease or recurrence of past sinus disease? The small radiolucency extending from the sinus floor through the buccal cortical plate could possibly be associated with the larger cyst-like lesion. The two most likely candidates were recurrent Odontogenic Keratocyst and an Ameloblastoma.
At this point, I requested that the referring dentist contact the patient to request 1) Had he had surgery, 2) What was the diagnosis?
The patient told the dentist that he had indeed had surgery, but he did not know the ultimate diagnosis. He thought it might be a cyst. I requested the dentist to contact the oral surgeon for a copy of the biopsy report. This was obtained and the report said the lesion appeared in parts to be a cystic ameloblastoma and possibly an odontogenic Keratocyst.
Now the radiographic appearance made sense. Both Ameloblastomas and Odontogenic Keratocysts have a risk of recurrence after surgery. Ameloblastomas that erode into soft tissue can be difficult to remove as the margins are hard to identify. Even though an ameloblastoma is a benign tumor, it is locally destructive so complete removal is important.
At this time, we do not have any further information about the cystic lesion. However, the point of this case study is to remind dentists:
- Please supply as much history as you have for past diseases and their treatments
- Radiologists will only know what you tell us about your patients

