

Region scanned: Maxilla
Reason for referral: Pre-implant assessment of the maxilla
Findings:
The edentulous regions have mild to moderate vertical bone resorption with moderate density cortical and trabecular bone. The UL7 edentulous ridge has a well-defined radiopacity measuring 4 x 3 x 6 mm, extending from the alveolar crest to the sinus floor. This is a dense bony island or retained root tip.
The UR3, UR1 and UL5 are root treated to apices with normal periodontal ligament spaces.
The UR4 is root treated. The buccal root filling is short of the apex with an apical radiolucency 3-4 mm wide. This is probably an apical granuloma or radicular cyst secondary to chronic apical periodontitis. The palatal root canal is filled to the apex with an apical radiolucency 0.5-1 mm wide.
The UL1 has external root resorption, mostly on the palatal side of the root. Approximately a third to half of the root is resorbed. There is no apical radiolucency but the root may be partially ankylosed to the bone. The UL2 also has external root resorption but to a lesser extent.
Both maxillary and left sphenoid sinuses have mild generalised thickening of the mucosal linings. There is no expansion or bony erosion of the sinus walls.
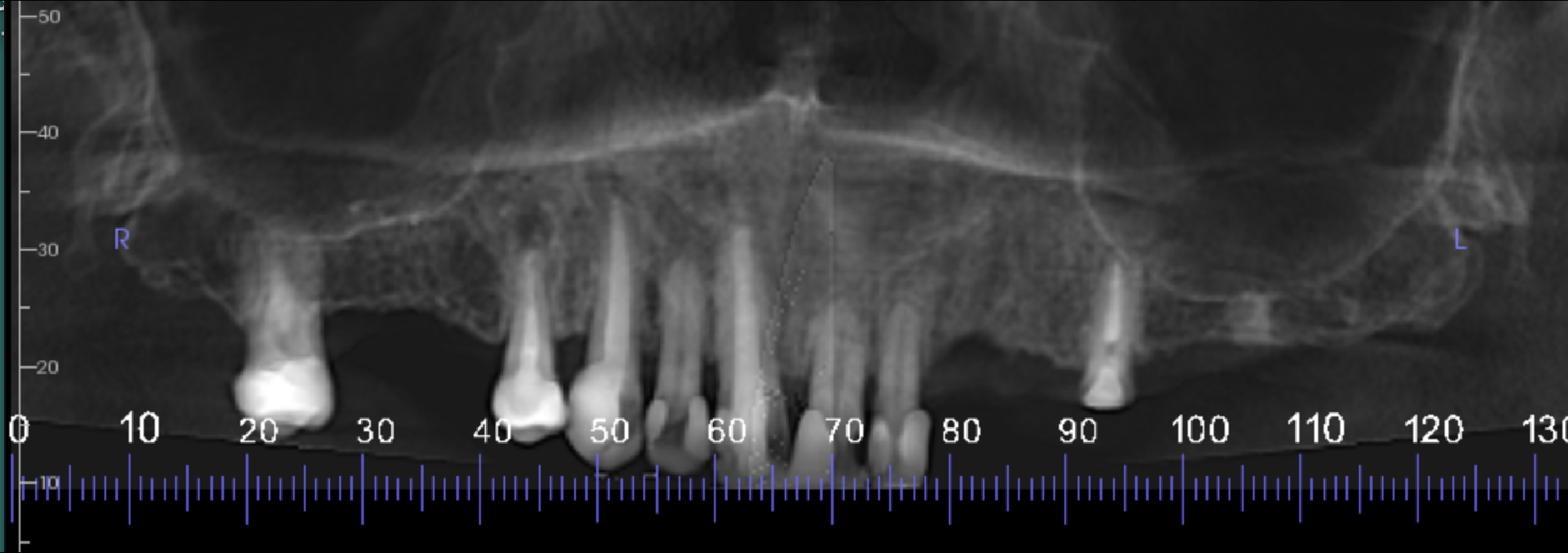
Reconstructed panoramic view of the maxilla
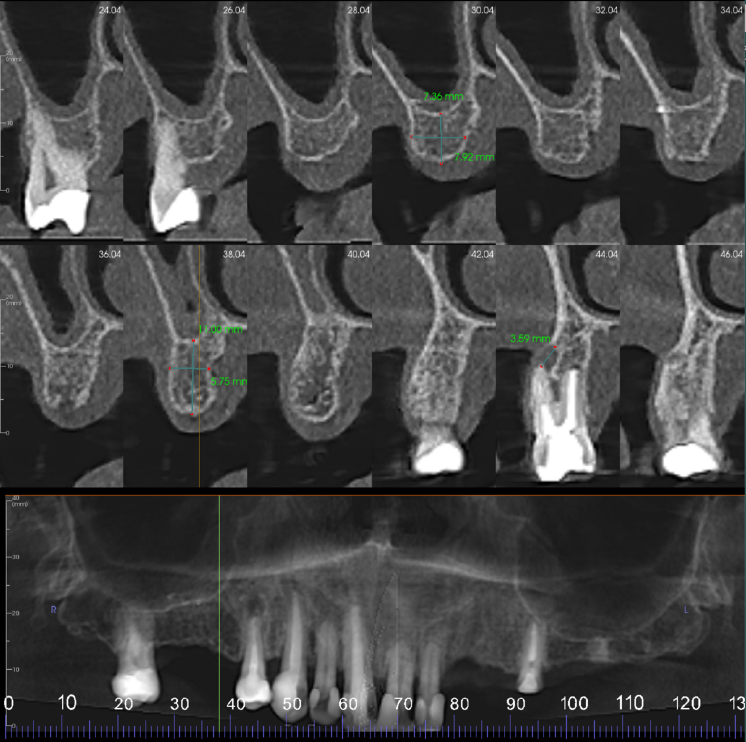
UR7-4 region cross sections at 2 mm intervals. Moderate loss in vertical bone height. The UR4 is root treated. The buccal root filling is short of the apex with 3-4 mm wide apical radiolucency. The palatal root canal is filled to the apex with 0.5-1 mm wide radiolucency

UL3-4 region cross sections at 3 mm intervals. Mild loss in vertical bone height. Moderate density cortical and trabeculae bone
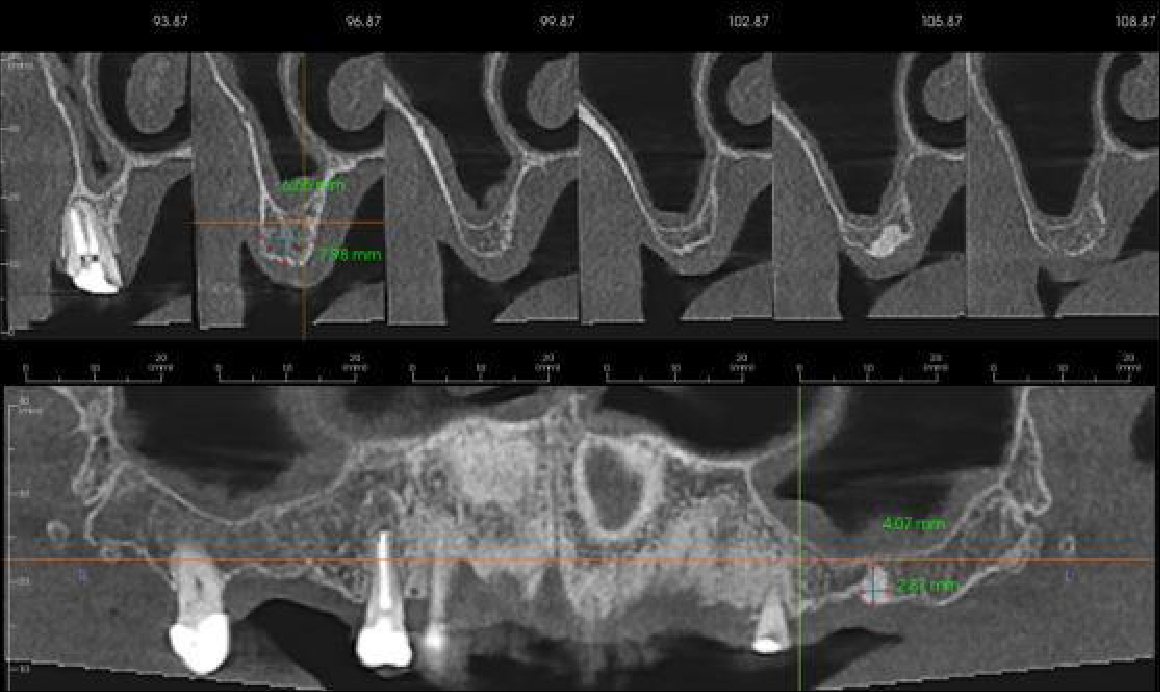
UL5-7 region cross sections at 3 mm intervals. Moderate loss in vertical bone height. Moderate density cortical and trabeculae bone
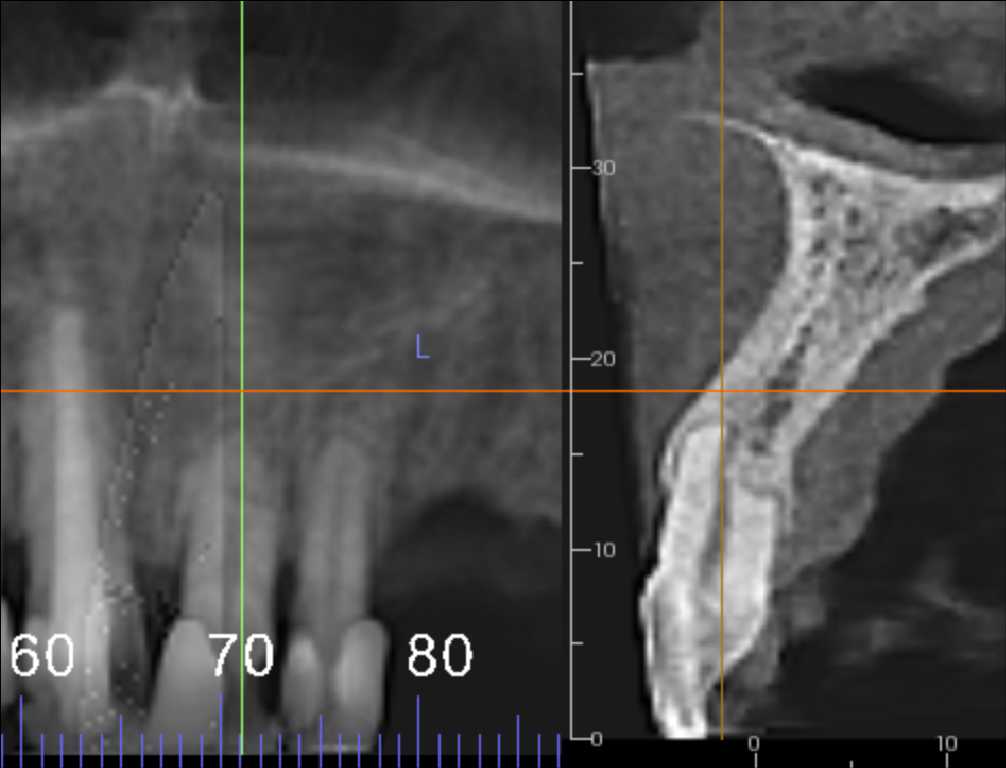
UL1 showing external root resorption, mostly on the palatal side of the root. Approximately a third to half of the root resorbed. The root may be partially ankylosed to the bone
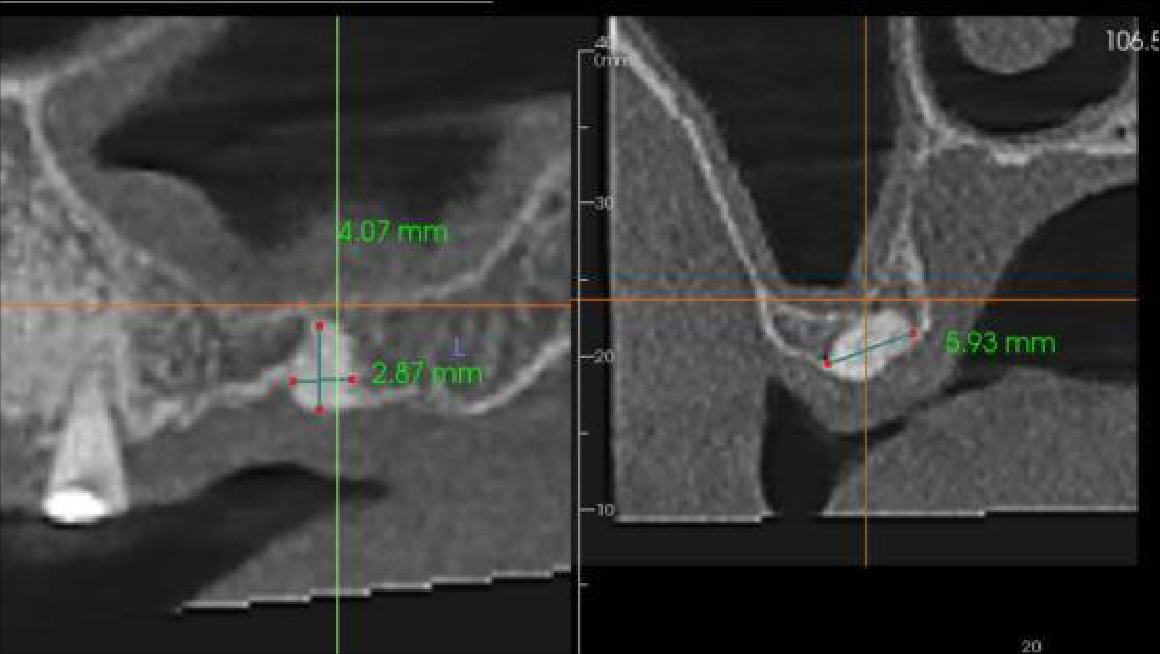
UL7 edentulous ridge. Well defined radiopacity extending from the alveolar bone crest to the sinus floor
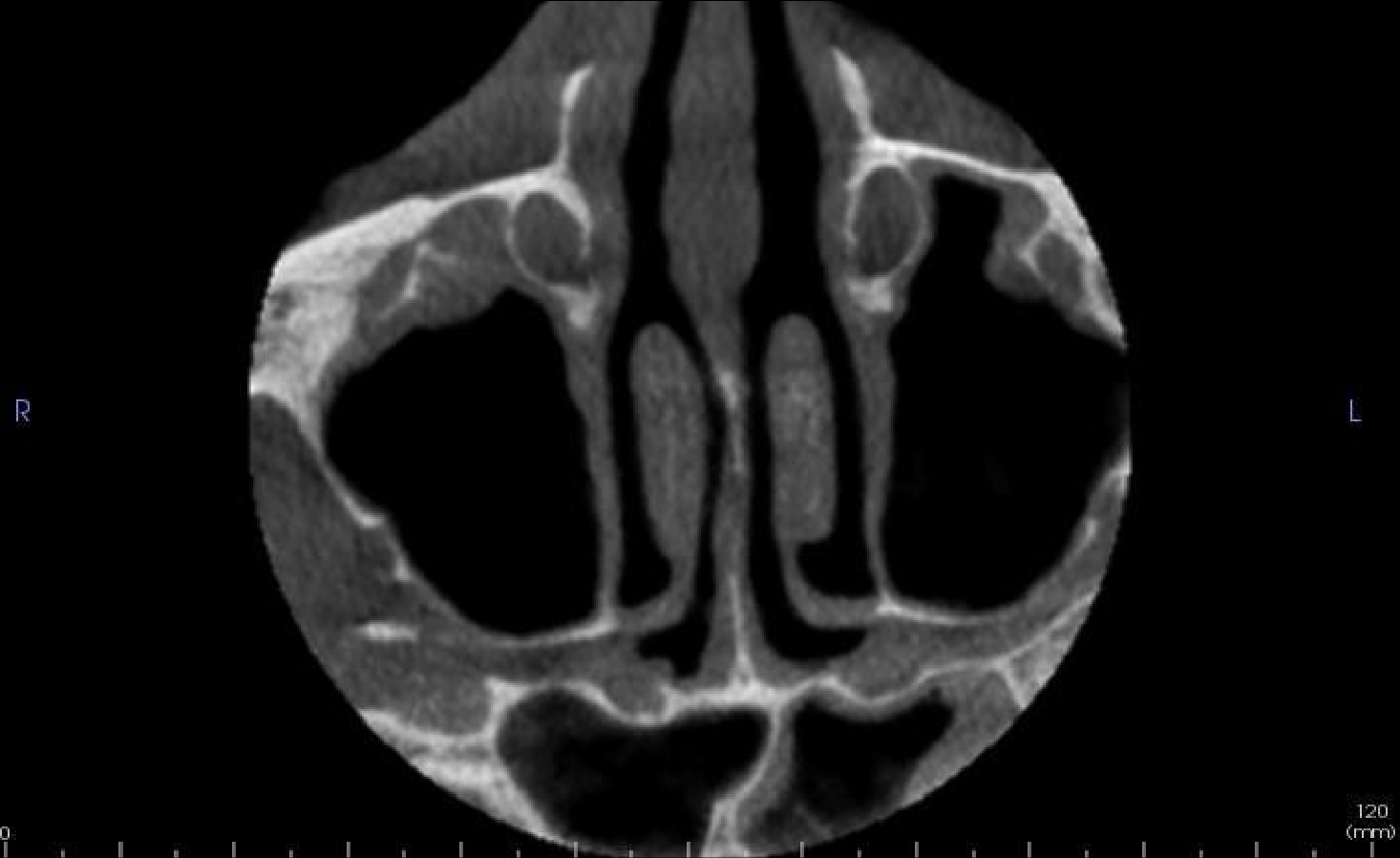

Axial and coronal slices showing mucosal lining thickening of the left sphenoid sinus
Learning from this case:
It is good practice to assess the entire data set systematically when clinically evaluating a CBCT scan. A thorough approach to examining the volume prompts appropriate management for the patient of any known or incidental findings.

